A blood test result sheet is one of the densest documents in medicine: 20 to 120 numbers, each with its own units, its own reference interval, and its own asterisk when something drifts out of range. Most people scan for the red flags, panic at one high value, and miss the quieter pattern sitting three lines away. This walkthrough teaches the opposite habit — reading your results the way a clinician does, and the way our analyzer, built on the Kantesti AI engine, does in under 60 seconds.
We will work through one realistic, anonymized report from top to bottom. By the end you will know how to read blood test results as connected stories rather than isolated numbers, which thresholds actually matter, and where an AI second read genuinely helps — and where it cannot replace your doctor.
Why patterns beat single values
Reference ranges are built so that about 95% of a healthy population falls inside them. That statistical design has a blunt consequence: roughly 5% of perfectly healthy people fall outside any given range by definition. On a 40-marker panel, pure chance means one or two flags are expected even when nothing is wrong. This is why a single out-of-range value, read alone, is one of the most over-interpreted things in consumer health.
The signal lives in the clusters. A mildly low hemoglobin means little by itself; low hemoglobin plus small red cells (low MCV) plus low ferritin is a coherent story — iron-deficiency anemia — with a cause worth chasing. The International Federation of Clinical Chemistry (IFCC) and the CALIPER and NORIP reference-interval studies exist precisely because context — age, sex, sometimes ethnicity and pregnancy — changes where the line should sit. A good reader, human or machine, holds all of that at once.

The core mindset
Never read a flagged value in isolation. Ask three questions: How far out of range is it? Which related markers move with it? And which way is it trending versus my last test?
Meet our sample report
Our worked example is a composite, not a real patient: a 34-year-old woman, no chronic diagnoses, who ordered a broad wellness panel because of six months of fatigue and feeling cold. Everything below is fabricated for teaching. Her panel covers a complete blood count (CBC), a metabolic panel with HbA1c, a lipid panel, thyroid function, iron studies, and vitamin D — the same 120+ biomarker families our analyzer maps to LOINC codes on upload.


Reading the CBC red-cell line
The complete blood count is where fatigue investigations usually start. Beginners fixate on hemoglobin alone; experienced readers read the whole red-cell line together — hemoglobin, hematocrit, red cell count, and the red-cell indices MCV (average cell size) and MCH. The indices are what tell you why a hemoglobin is low. Our full CBC explainer goes deeper, but here is the pattern that matters.

Read as a group, this is not five separate abnormalities — it is one finding. The hemoglobin is mildly low, the cells are small (MCV 74 fL, below the ~80 fL floor) and under-hemoglobinized (low MCH). That triad defines a microcytic anemia, and in a menstruating adult the overwhelmingly common cause is iron deficiency. Note what a single-value reader would miss: platelets nudging the high end are a recognized reactive companion of iron deficiency, not a second unrelated problem. The pattern ties the sheet together.
The number that changes management is rarely the one the patient is most worried about. It is usually the quiet index sitting next to it.
— Dr. Sophie Laurent, MD MPH, Hematology, Penn
Glucose, HbA1c and the metabolic panel
The comprehensive metabolic panel covers glucose, kidney markers (creatinine, eGFR, BUN), electrolytes, and liver enzymes. For most wellness readers the headline is glycemic status, and the durable number there is HbA1c — a rough average of blood sugar over the prior ~3 months, less jumpy than a single fasting glucose. The American Diabetes Association (ADA) Standards of Care are unambiguous on the cutoffs, so memorize them.
| HbA1c | Category (ADA) | What it means |
|---|---|---|
| Below 5.7% | Normal | No action beyond routine screening |
| 5.7% to 6.4% | Prediabetes | Lifestyle change; retest; discuss risk |
| 6.5% or higher | Diabetes range | Needs clinician confirmation and workup |
Our patient's HbA1c is 5.4% and fasting glucose 91 mg/dL — both comfortably normal. Her liver enzymes and eGFR are unremarkable. This is exactly the kind of result an anxious reader can waste worry on, because a fasting glucose of, say, 99 mg/dL looks 'high' next to a round number even though it is normal. Reading HbA1c and glucose together, against ADA thresholds, settles it fast. Our HbA1c guide covers the edge cases — anemia and hemoglobin variants can distort HbA1c, which is itself a reason to read it alongside the CBC rather than alone.

Making sense of the lipid panel
The lipid panel reports total cholesterol, LDL ('bad') cholesterol, HDL ('good') cholesterol, and triglycerides. The critical nuance most patients miss: there is no single universal LDL cut-off. The right target depends on your overall cardiovascular risk. Drawing on AHA/ACC and European Society of Cardiology (ESC) lipid guidance, a workable mental model is: below 100 mg/dL is a reasonable general goal, below 70 mg/dL for high-risk individuals, and below 55 mg/dL for people with established cardiovascular disease.

Her LDL of 118 mg/dL is above the general 100 mg/dL goal but not dramatically so; triglycerides at 165 mg/dL are mildly elevated; HDL is on the low side of desirable. No single value screams. Read as a cluster, this is a borderline dyslipidemia — the province of diet, activity, and a repeat test in a few months for a healthy 34-year-old, and a conversation about absolute risk rather than an automatic prescription. Our lipid panel guide walks through how risk calculators shift these targets. The key teaching point: without knowing her risk category, no honest reader can convert 118 mg/dL into a verdict — the number is meaningless out of context.
Fasting still matters for triglycerides
Triglycerides and, to a lesser degree, glucose are sensitive to whether you fasted. A non-fasting draw can push triglycerides up. Always check whether your report notes fasting status before interpreting a borderline triglyceride.
Thyroid, iron and vitamin D
Fatigue and cold intolerance make the thyroid a natural suspect, so this panel earns a careful read. TSH is the screening workhorse, with a common reference interval of roughly 0.4 to 4.0 mIU/L per American Thyroid Association and Endocrine Society guidance. TSH moves inversely to thyroid hormone: a high TSH suggests an underactive gland. Our patient's TSH is 2.6 mIU/L with a normal free T4 — thyroid is not her problem, an important thing to rule out cleanly. See our thyroid panel guide for subclinical cases where TSH is mildly high but free T4 is still normal.
Iron studies are where her CBC story gets confirmed. Ferritin — the body's iron store — is the most useful single marker, though it rises with inflammation, so it is read alongside serum iron and transferrin saturation. A low ferritin with low transferrin saturation, on top of a microcytic anemia, closes the loop on iron-deficiency anemia.

On vitamin D, the widely used thresholds define deficiency as below 20 ng/mL, with 20 to 30 ng/mL commonly labeled insufficient and 30+ ng/mL sufficient. Her 22 ng/mL is insufficient rather than frankly deficient — a nudge toward review, sunlight and possibly supplementation, not an emergency. Our vitamin D explainer covers why labs disagree at the margins. Two mild findings — low iron stores and low-ish vitamin D — that individually look minor together explain a great deal of her six months of fatigue.

How an AI analyzer reads it all together
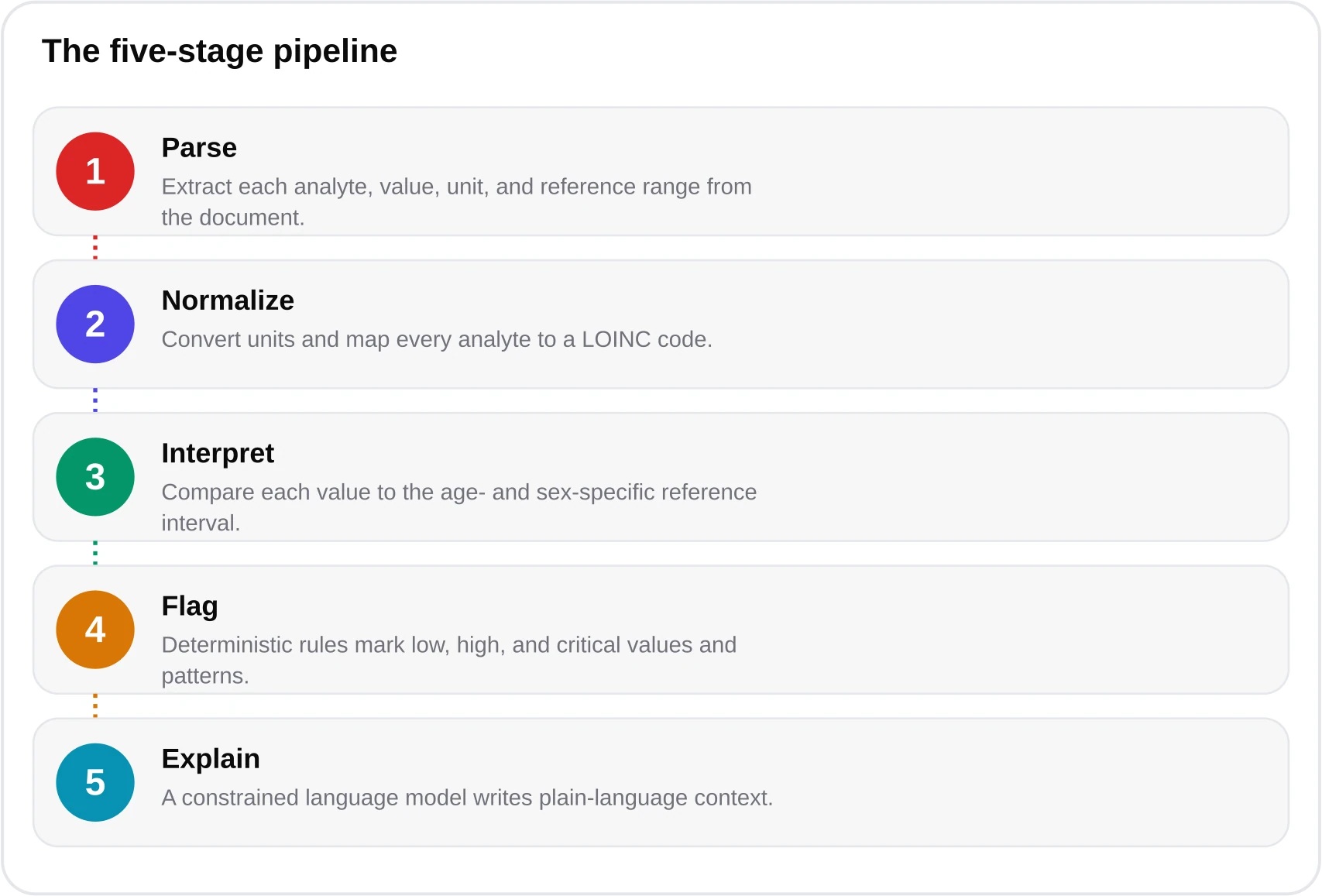
Here is where machine reading earns its place. A human eye, moving line by line, is prone to anchoring on the first flag and tiring by line 40. An AI analyzer extracts every value at once, normalizes units, maps each result to its LOINC code, and applies age- and sex-specific reference partitions drawn from CALIPER and NORIP plus CDC 2024 data — before any interpretation happens. Our system pairs the health-llm-v4.7 model with a deterministic clinical-rules engine, so the pattern-spotting is grounded in fixed thresholds rather than a model's free improvisation. You can see the mechanics in our how-it-works page and the validation detail in our methodology.

For this report the analyzer surfaced the microcytic-anemia cluster, tied the low ferritin to it, separately flagged the vitamin D insufficiency, labeled the lipids borderline with a note that the LDL target depends on cardiovascular risk, and explicitly cleared the thyroid and glycemic panels. That is exactly how a clinician triages: group, rank, and separate 'act now' from 'watch'. The tool is not diagnosing — it is organizing. If you want to try the same read on your own report, the beta analyzer is free at kantesti.net/free-blood-test, and our walkthrough series pairs with the AI analysis overview for the underlying method.

A word on limits, because honesty is the whole point of an EEAT-first read. blood-test.life is not a medical device and does not diagnose. It reads what is on the page; it cannot examine you, know your symptoms unless you tell it, or order the follow-up tests a real workup needs. It will not tell our patient why she is iron deficient — the essential next question — because that requires a clinician. Your files are deleted after delivery, never used for training, and the system is HIPAA-aligned and GDPR/CCPA-compliant, but privacy is not a substitute for a doctor. Treat the AI read as a fast, well-organized first pass, then take it to a professional.
Turning results into a doctor conversation
The payoff of reading well is a sharper appointment. Instead of 'my cholesterol looked high,' our patient can say: 'I have a microcytic anemia with a ferritin of 9, insufficient vitamin D at 22, and borderline lipids — can we work out the cause of the iron loss and decide whether my LDL needs anything given my risk?' That is a five-minute visit that actually moves. Trends matter as much as any single visit, so bring prior results if you have them.

Notice the sequence in that trend: iron stores fell first, and the hemoglobin only followed once the reserve ran out. That is textbook iron deficiency evolving into anemia, and it is invisible on a single report. This is the strongest argument for keeping your results in one place and re-reading them over time — something an analyzer that ingests old and new reports does naturally.

Reading blood work is a learnable skill: match to the right reference range, read in clusters, weigh borderline against trend, and separate what to watch from what to escalate. AI makes the mechanical part — extraction, unit conversion, range-matching across 120+ markers — fast and consistent, and it is honest about where its job ends and your clinician's begins. Start with the lab test analyzer overview, run your own report through the free beta, and bring the organized result to the person who can actually examine you.
Frequently asked questions
How do I know if a blood test value is actually a problem?
Check three things before worrying: how far outside the age- and sex-specific reference range it sits, whether related markers move with it, and how it compares to your previous results. A single mildly abnormal value on a large panel is statistically expected — about 5% of healthy people fall outside any given range — so context and clustering matter far more than one flag.
What is the difference between HbA1c and fasting glucose?
Fasting glucose is a single snapshot of blood sugar, while HbA1c reflects roughly a three-month average and is less affected by what you ate that morning. Per ADA criteria, HbA1c of 5.7-6.4% indicates prediabetes and 6.5% or higher is in the diabetes range. Because anemia and hemoglobin variants can distort HbA1c, it is best read alongside the CBC.
Can an AI blood test analyzer diagnose me?
No. blood-test.life is not a medical device and does not diagnose. It extracts every biomarker, applies age- and sex-specific reference ranges, and flags patterns to help you understand your results and prepare for a doctor visit. It cannot examine you or order follow-up tests, so any meaningful finding should be reviewed with a licensed clinician.
Why does my LDL cholesterol target differ from someone else's?
Because the right LDL goal depends on your overall cardiovascular risk. AHA/ACC and ESC guidance point to roughly below 100 mg/dL as a general goal, below 70 mg/dL for high-risk individuals, and below 55 mg/dL for people with established cardiovascular disease. A borderline LDL cannot be judged without knowing your risk category.
What does low ferritin with a normal-looking hemoglobin mean?
Ferritin measures your iron stores, which deplete before hemoglobin falls. A low ferritin with a still-normal hemoglobin often means early iron deficiency — the reserve is running down but anemia has not yet appeared. Watching ferritin over time can catch iron deficiency months before a routine CBC would flag it.
Is it safe to upload my lab report to an AI analyzer?
blood-test.life deletes uploaded files after your report is delivered, never trains on user data, and is HIPAA-aligned with GDPR and CCPA compliance. That said, privacy protections do not replace medical care — use the analyzer as a fast, organized first read, then take the results to a clinician who can act on them.
References & sources
- American Diabetes Association — Standards of Care in Diabetes (HbA1c criteria) — ADA
- American Heart Association / American College of Cardiology — Blood Cholesterol Guideline — AHA/ACC
- European Society of Cardiology — Dyslipidaemias Guidelines (LDL targets) — ESC
- American Thyroid Association — TSH and thyroid function testing — ATA
- National Heart, Lung, and Blood Institute — anemia and iron deficiency — NHLBI
- CDC — National Health and Nutrition data (reference population, 2024) — CDC
- LOINC — Logical Observation Identifiers Names and Codes — LOINC
- CALIPER and NORIP pediatric and Nordic reference-interval studies — IFCC reference-interval literature
Medical disclaimer
This article is informational and educational only and is not a substitute for professional medical advice, diagnosis, or treatment. blood-test.life is not a medical device. Always consult your physician or a qualified health provider about your results. Read our full medical disclaimer.